Overview
Plantar calcaneal bursitis is a medical condition in which there is inflammation of the plantar calcaneal bursa, a spongy fluid filled sac that cushions the fascia of the heel and the calcaneus (heel bone). It is characterized by swelling and tenderness of the central plantar heel area. It is sometimes called 'Policeman's heel'. It sometimes was, and should not be, confused with plantar fasciitis, which is inflammation of the plantar fascia and can affect any part of the foot.
Causes
Repetitive, vigorous movement, strenuous and unaccustomed activities that put pressure on a joint, or a blow or other injury can bring on bursitis. The cause can vary depending on where the bursitis occurs. In the shoulder, for example, it can be brought on by excessive strain, such as from serving in tennis. Kneeling on a hard floor can cause bursitis of the knee, and similarly, repeatedly resting the elbow on a hard surface (such as a desk) can cause bursitis in that joint. Arthritis, gout, and certain infections can also contribute to the problem. Bursitis, in fact, may signal the onset of arthritis. While getting older isn't a cause of bursitis, older people, especially older athletes, are more likely to develop the condition.
Symptoms
Symptoms of bursitis usually occur after rest and relaxation. Upon activity there is usually more intense pain in the area of the bursa. The common areas to have a bursitis in the foot are in the bottom of the heel, behind the heel near the attachment of the Achilles Tendon as well as along the side of a bunion. A bursa may also form in multiple areas especially along the metatarsal heads, or "ball" of your foot. You may actually feel the sac like fluid when rubbing the area of pain.
Diagnosis
Carrying out a diagnosis for bursitis is fairly straightforward. The doctor will examine the affected area and ask the patient some questions about his/her recent activities. If the patient has a high temperature the physician may take a small sample of fluid from a bursa near the affected body part. The sample will be tested for bacteria, and perhaps also crystals. If the patient does not get better after treatment the doctor may carry out further tests so that he/she can eliminate the possibility that the symptoms might not be due to something else. These may include an x-ray, to make sure no bones are broken or fractured. Blood tests, to check for rheumatoid arthritis. A CT scan or MRI scan to see if there is a torn tendon.
Non Surgical Treatment
So what can you do to alleviate this type of pain in the foot? If the bursitis pain is occurring on the toes, bunion or back of the heel area the smart money would be on eliminating the shoes that seem to aggravate the condition. Eliminating these shoes may not in itself clear up the problem but you can be sure that if you continue to wear the offending shoes nothing you or your doctor do will permanently ?fix? the problem. A recurring theme that I use throughout this site that if you put an abnormally shaped foot in a dressy shoe it is literally the same as trying to put a square peg in a round hole, it will not fit. OK, so you threw away those dressy shoes and the foot still hurts, now what? Depending on the severity of the pain, over the counter anti-inflammatory medication may do the trick. The key here is to take the medication on an ongoing basis, according to the directions on the package to build up therapeutic blood levels. Assuming you can tolerate this type of medication, along with alternative treatments you can try). take the medication for 10-14 days. Stop if the symptoms have not dramatically improved. Icing the area during this period may also help reduce the symptoms.
Surgical Treatment
Bursectomy is a surgical procedure used to remove an inflamed or infected bursa, which is a fluid-filled sac that reduces friction between tissues of the body. Because retrocalcaneal bursitis can cause chronic inflammation, pain and discomfort, bursectomy may be used as a treatment for the condition when it is persistent and cannot be relived with other treatments. During this procedure, a surgeon makes small incisions so that a camera may be inserted into the joint. This camera is called an arthroscope. Another small incision is made so that surgical instruments can be inserted to remove the inflamed bursa.
Plantar calcaneal bursitis is a medical condition in which there is inflammation of the plantar calcaneal bursa, a spongy fluid filled sac that cushions the fascia of the heel and the calcaneus (heel bone). It is characterized by swelling and tenderness of the central plantar heel area. It is sometimes called 'Policeman's heel'. It sometimes was, and should not be, confused with plantar fasciitis, which is inflammation of the plantar fascia and can affect any part of the foot.
Causes
Repetitive, vigorous movement, strenuous and unaccustomed activities that put pressure on a joint, or a blow or other injury can bring on bursitis. The cause can vary depending on where the bursitis occurs. In the shoulder, for example, it can be brought on by excessive strain, such as from serving in tennis. Kneeling on a hard floor can cause bursitis of the knee, and similarly, repeatedly resting the elbow on a hard surface (such as a desk) can cause bursitis in that joint. Arthritis, gout, and certain infections can also contribute to the problem. Bursitis, in fact, may signal the onset of arthritis. While getting older isn't a cause of bursitis, older people, especially older athletes, are more likely to develop the condition.
Symptoms
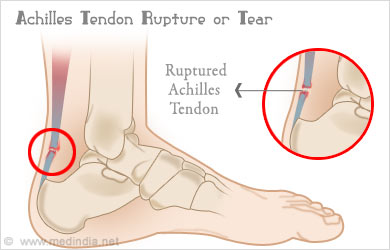
Symptoms of bursitis usually occur after rest and relaxation. Upon activity there is usually more intense pain in the area of the bursa. The common areas to have a bursitis in the foot are in the bottom of the heel, behind the heel near the attachment of the Achilles Tendon as well as along the side of a bunion. A bursa may also form in multiple areas especially along the metatarsal heads, or "ball" of your foot. You may actually feel the sac like fluid when rubbing the area of pain.
Diagnosis
Carrying out a diagnosis for bursitis is fairly straightforward. The doctor will examine the affected area and ask the patient some questions about his/her recent activities. If the patient has a high temperature the physician may take a small sample of fluid from a bursa near the affected body part. The sample will be tested for bacteria, and perhaps also crystals. If the patient does not get better after treatment the doctor may carry out further tests so that he/she can eliminate the possibility that the symptoms might not be due to something else. These may include an x-ray, to make sure no bones are broken or fractured. Blood tests, to check for rheumatoid arthritis. A CT scan or MRI scan to see if there is a torn tendon.
Non Surgical Treatment
So what can you do to alleviate this type of pain in the foot? If the bursitis pain is occurring on the toes, bunion or back of the heel area the smart money would be on eliminating the shoes that seem to aggravate the condition. Eliminating these shoes may not in itself clear up the problem but you can be sure that if you continue to wear the offending shoes nothing you or your doctor do will permanently ?fix? the problem. A recurring theme that I use throughout this site that if you put an abnormally shaped foot in a dressy shoe it is literally the same as trying to put a square peg in a round hole, it will not fit. OK, so you threw away those dressy shoes and the foot still hurts, now what? Depending on the severity of the pain, over the counter anti-inflammatory medication may do the trick. The key here is to take the medication on an ongoing basis, according to the directions on the package to build up therapeutic blood levels. Assuming you can tolerate this type of medication, along with alternative treatments you can try). take the medication for 10-14 days. Stop if the symptoms have not dramatically improved. Icing the area during this period may also help reduce the symptoms.
Surgical Treatment
Bursectomy is a surgical procedure used to remove an inflamed or infected bursa, which is a fluid-filled sac that reduces friction between tissues of the body. Because retrocalcaneal bursitis can cause chronic inflammation, pain and discomfort, bursectomy may be used as a treatment for the condition when it is persistent and cannot be relived with other treatments. During this procedure, a surgeon makes small incisions so that a camera may be inserted into the joint. This camera is called an arthroscope. Another small incision is made so that surgical instruments can be inserted to remove the inflamed bursa.
 Overview
Overview Symptoms
Symptoms Prevention
Prevention










 The most common cause of heel pain is plantar fasciitis. It is usually caused by a biomechanical imbalance resulting in tension along the plantar fascia. The diagnosis is typically based on the history and the finding of localized tenderness. Treatment consists of medial arch support, anti-inflammatory medications, ice massage and stretching. Corticosteroid injections and casting may also be tried. Surgical fasciotomy should be reserved for use in patients in whom conservative measures have failed despite correction of biomechanical abnormalities. Heel pain may also have a neurologic, traumatic or systemic origin. I have a red, sore lump on the back of my heel. Is that what they call a “pump bump”? There are many causes behind the heel pain. It’s like an enemy to our daily life. Some how it may be a good sign that if it occurs in our early life that could warn us for having a protective treatment. Heel pain may happen due to our defective biomechanics which could cause much stress on the heel bones and the elastic tissues close to it. The root causes of it can be running or jumping on the hard floors, wearing defective or poorly constructed footwear, any injury to heel bone or carrying surfeit weights. These concrete structures have to keep us stand on our feet. Many of us think that foot problems are one of the aches and pains of aging. But heel pain is not normal nor is it isolated to only adults. I have seen my share fair of children and teens that are having difficulty playing sports or participating in gym classes because of heel pain! Sever's disease is the most common cause of childhood heel pain and usually affects children 8-14 years of age Try to incorporate regular stretching, increasing the range of motion and functional exercise. Waling is ideal for foot health. Exercise will help to improve blood flow to the feet, improve flexibility and keep bones and muscles strong. Nearly 40 percent of Americans revealed foot pain has inhibited them from performing life’s daily activities. Foot pain is never normal. If you experience foot pain, see your podiatric physician immediately. Heel Pain Videos What is Plantar Fasciitis and How Can I Treat It? Heel pain treatment is effective, and leads to long lasting relief when done properly. That is where we fit in. Our doctors are highly experienced in treating heel pain, and can give you your life back. Scroll to the bottom of this page for common Frequently Asked Questions, and use the FAQs tab on the top of the page to find an ever expanding list !
The most common cause of heel pain is plantar fasciitis. It is usually caused by a biomechanical imbalance resulting in tension along the plantar fascia. The diagnosis is typically based on the history and the finding of localized tenderness. Treatment consists of medial arch support, anti-inflammatory medications, ice massage and stretching. Corticosteroid injections and casting may also be tried. Surgical fasciotomy should be reserved for use in patients in whom conservative measures have failed despite correction of biomechanical abnormalities. Heel pain may also have a neurologic, traumatic or systemic origin. I have a red, sore lump on the back of my heel. Is that what they call a “pump bump”? There are many causes behind the heel pain. It’s like an enemy to our daily life. Some how it may be a good sign that if it occurs in our early life that could warn us for having a protective treatment. Heel pain may happen due to our defective biomechanics which could cause much stress on the heel bones and the elastic tissues close to it. The root causes of it can be running or jumping on the hard floors, wearing defective or poorly constructed footwear, any injury to heel bone or carrying surfeit weights. These concrete structures have to keep us stand on our feet. Many of us think that foot problems are one of the aches and pains of aging. But heel pain is not normal nor is it isolated to only adults. I have seen my share fair of children and teens that are having difficulty playing sports or participating in gym classes because of heel pain! Sever's disease is the most common cause of childhood heel pain and usually affects children 8-14 years of age Try to incorporate regular stretching, increasing the range of motion and functional exercise. Waling is ideal for foot health. Exercise will help to improve blood flow to the feet, improve flexibility and keep bones and muscles strong. Nearly 40 percent of Americans revealed foot pain has inhibited them from performing life’s daily activities. Foot pain is never normal. If you experience foot pain, see your podiatric physician immediately. Heel Pain Videos What is Plantar Fasciitis and How Can I Treat It? Heel pain treatment is effective, and leads to long lasting relief when done properly. That is where we fit in. Our doctors are highly experienced in treating heel pain, and can give you your life back. Scroll to the bottom of this page for common Frequently Asked Questions, and use the FAQs tab on the top of the page to find an ever expanding list !  RSS Feed
RSS Feed