Overview

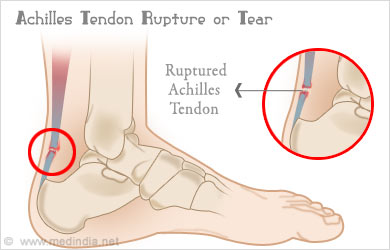
Your Achilles tendon is a large band of tissue in the back of your ankle. It connects your calf muscles to your heel bone. The tendon helps you point your foot downward, rise on your toes, and push off when you walk. You use it almost every time you move. But repeated stress can make the tendon more prone to injury. It may become inflamed and develop small tears (tendonitis). A complete tear through the tendon is known as an Achilles tendon rupture.
Causes
The Achilles tendon usually ruptures as a result of a sudden forceful contraction of the calf muscles. Activities such as jumping, lunging, or sprinting can cause undue stress on the Achilles tendon and cause it to rupture. Often there is a background of Achilles tendinitis. Direct trauma to the area, poor flexibility or weakness of the calf muscles or of the Achilles tendon and increasing age are some of the other factors that are associated with an Achilles tendon rupture.
Symptoms
Patients with an Achilles tendon rupture frequently present with complaints of a sudden snap in the lower calf associated with acute, severe pain. The patient reports feeling like he or she has been shot, kicked, or cut in the back of the leg, which may result in an inability to ambulate further. A patient with Achilles tendon rupture will be unable to stand on his or her toes on the affected side.
Diagnosis
If an Achilles tendon rupture is suspected, it is important to consult a doctor straight away so that an accurate diagnosis can be made and appropriate treatment recommended. Until a doctor can be consulted it is important to let the foot hang down with the toes pointed to the ground. This prevents the ends of the ruptured tendon pulling any farther apart. The doctor will take a full medical history, including any previous Achilles tendon injuries and what activity was being undertaken at the time the present injury occurred. The doctor will also conduct a physical examination and will check for swelling, tenderness and range of movement in the lower leg and foot. A noticeable gap may be able to be felt in the tendon at the site of the rupture. This is most obvious just after the rupture has occurred and swelling will eventually make this gap difficult to feel. One test commonly used to confirm an Achilles tendon rupture is the Thomson test. For this test the patient lies face down on an examination table. The doctor then squeezes the calf muscles; an action that would normally cause the foot to point like a ballerina (plantar flexion). When a partial rupture has occurred the foot's ability to point may be decreased. When a complete rupture has occurred, the foot may not point at all. Ultrasound scanning of the Achilles tendon may also be recommended in order to assist with the diagnosis.
Non Surgical Treatment
Medical therapy for a patient with an Achilles tendon rupture consists of rest, pain control, serial casting, and rehabilitation to maximize function. Ongoing debate surrounds the issue of whether medical or surgical therapy is more appropriate for this injury. Conservative management of Achilles tendinosis and paratenonitis includes the following. Physical therapy. Eccentric exercises are the cornerstone of strengthening treatment, with most patients achieving 60-90% pain relief. Orthotic therapy in Achilles tendinosis consists of the use of heel lifts. Nonsteroidal anti-inflammatory drugs (NSAIDs). Tendinosis tends to be less responsive than paratenonitis to NSAIDs. Steroid injections. Although these provide short-term relief of painful symptoms, there is concern that they can weaken the tendon, leading to rupture. Vessel sclerosis. Platelet-rich plasma injections. Nitric oxide. Shock-wave therapy.
Surgical Treatment
Surgery to repair an Achilles tendon rupture is performed under a spinal or general anaesthetic. During surgery the surgeon makes an incision in the skin over the ruptured portion of the tendon. The tendon ends are located and joined together with strong sutures (stitches), allowing the tendon to closely approximate its previous length. The skin is then closed with sutures and the foot is immobilised in a cast or splint, again in the toes-pointed position. Seven to ten days after surgery the cast or splint is removed in order for the sutures in the skin to be removed. Another cast or splint will be applied and will stay in place a further 5 - 7 weeks.
Your Achilles tendon is a large band of tissue in the back of your ankle. It connects your calf muscles to your heel bone. The tendon helps you point your foot downward, rise on your toes, and push off when you walk. You use it almost every time you move. But repeated stress can make the tendon more prone to injury. It may become inflamed and develop small tears (tendonitis). A complete tear through the tendon is known as an Achilles tendon rupture.
Causes
The Achilles tendon usually ruptures as a result of a sudden forceful contraction of the calf muscles. Activities such as jumping, lunging, or sprinting can cause undue stress on the Achilles tendon and cause it to rupture. Often there is a background of Achilles tendinitis. Direct trauma to the area, poor flexibility or weakness of the calf muscles or of the Achilles tendon and increasing age are some of the other factors that are associated with an Achilles tendon rupture.
Symptoms
Patients with an Achilles tendon rupture frequently present with complaints of a sudden snap in the lower calf associated with acute, severe pain. The patient reports feeling like he or she has been shot, kicked, or cut in the back of the leg, which may result in an inability to ambulate further. A patient with Achilles tendon rupture will be unable to stand on his or her toes on the affected side.
Diagnosis
If an Achilles tendon rupture is suspected, it is important to consult a doctor straight away so that an accurate diagnosis can be made and appropriate treatment recommended. Until a doctor can be consulted it is important to let the foot hang down with the toes pointed to the ground. This prevents the ends of the ruptured tendon pulling any farther apart. The doctor will take a full medical history, including any previous Achilles tendon injuries and what activity was being undertaken at the time the present injury occurred. The doctor will also conduct a physical examination and will check for swelling, tenderness and range of movement in the lower leg and foot. A noticeable gap may be able to be felt in the tendon at the site of the rupture. This is most obvious just after the rupture has occurred and swelling will eventually make this gap difficult to feel. One test commonly used to confirm an Achilles tendon rupture is the Thomson test. For this test the patient lies face down on an examination table. The doctor then squeezes the calf muscles; an action that would normally cause the foot to point like a ballerina (plantar flexion). When a partial rupture has occurred the foot's ability to point may be decreased. When a complete rupture has occurred, the foot may not point at all. Ultrasound scanning of the Achilles tendon may also be recommended in order to assist with the diagnosis.
Non Surgical Treatment
Medical therapy for a patient with an Achilles tendon rupture consists of rest, pain control, serial casting, and rehabilitation to maximize function. Ongoing debate surrounds the issue of whether medical or surgical therapy is more appropriate for this injury. Conservative management of Achilles tendinosis and paratenonitis includes the following. Physical therapy. Eccentric exercises are the cornerstone of strengthening treatment, with most patients achieving 60-90% pain relief. Orthotic therapy in Achilles tendinosis consists of the use of heel lifts. Nonsteroidal anti-inflammatory drugs (NSAIDs). Tendinosis tends to be less responsive than paratenonitis to NSAIDs. Steroid injections. Although these provide short-term relief of painful symptoms, there is concern that they can weaken the tendon, leading to rupture. Vessel sclerosis. Platelet-rich plasma injections. Nitric oxide. Shock-wave therapy.
Surgical Treatment
Surgery to repair an Achilles tendon rupture is performed under a spinal or general anaesthetic. During surgery the surgeon makes an incision in the skin over the ruptured portion of the tendon. The tendon ends are located and joined together with strong sutures (stitches), allowing the tendon to closely approximate its previous length. The skin is then closed with sutures and the foot is immobilised in a cast or splint, again in the toes-pointed position. Seven to ten days after surgery the cast or splint is removed in order for the sutures in the skin to be removed. Another cast or splint will be applied and will stay in place a further 5 - 7 weeks.
 RSS Feed
RSS Feed